

Introduction
As the COVID-19 pandemic spread throughout the world, it was seen that patients who presented with critical disease had a higher incidence of thrombotic complications, associated with a poor prognosis. Currently prophylactic anticoagulation is recommended for all patients with COVID-19 who require hospitalization as part of the supportive management. However, since a higher incidence of thrombosis despite prophylactic anticoagulation has been reported, some recommendations indicate that an increase to intermediate or therapeutic dosing should be considered. The full spectrum of complications and outcomes related to this strategy are still unknown.
Methods
We conducted a cross-sectional study using the COVID-19 registry of the ARMII study group, based in Centro Medico ABC, a private hospital in Mexico City. We included all patients admitted from March 12 to July 31, 2020, who received prophylactic anticoagulation at standard (enoxaparin 40mg QD), intermediate (0.5 mg/kg QD or 40 mg BID), or therapeutic doses (1mg/kg BID), a decision taken by the attending physician based on clinical and laboratory criteria. Patients with previous or presenting with thrombosis were excluded.
We compared the three groups to identify baseline characteristics and conducted multivariable logistic regressions to measure the association of anticoagulation profiles and adverse outcomes.
Results
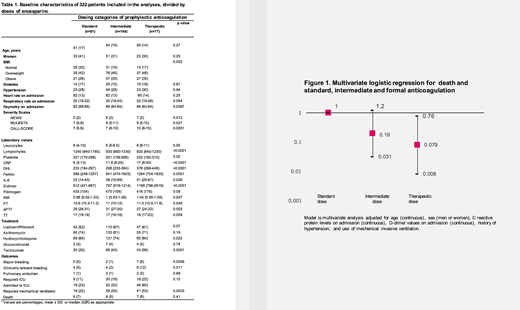
Out of total 322 patients, we identified 81 (25%) who received standard dose, 164 (51%) who received intermediate and 77 (24%) on therapeutic doses. Age and sex were distribuited similarly among groups; patients with intermediate and therapeutic doses were more overweight and obese, but this was not significant (p=0.052). On admission, patients who received intermediate and therapeutic doses had lower oximetry registry when compared with standard doses (89%, 88% and 92% respectively, p=0.008). Three severity scales, NEWS, MULBSTA and CALL, were higher in patients with intermediate and therapeutic doses (p=0.01, p=0.02 and p=0.005, respectively). Regarding laboratory values, patients on therapeutic doses had higher leucocytes on admission (median 6 x 109L, 6 and 8, p=0.05) but lower lymphocyte absolute counts (median 1240 cells/mm3, 935 and 920, p<0.001). Patients who were given higher doses of anticoagulation had higher levels of C-reactive protein, DHL, and ferritin (p<0.001) and higher levels of IL-6 (p=0.02). Levels of D-dimer were also higher in this group (p<0.001). Patients with therapeutic doses of anticoagulation were more likely to present major bleeding when compared to intermediate or standard prophylactic doses (9% vs 1% vs 0%, p=0.0006) and clinically relevant bleeding (12% vs 2% vs 5%, p=0.01).
(Table 1)
The incidence of pulmonary embolism (PE) in the entire cohort was 5%, while the incidence of major bleeding was 2.5%. There were no differences between the different doses of anticoagulation; no patients presented deep venous thrombosis.
During follow-up, a total of 21 patients died, representing 6.5% of the study population. Independent factors that predicted death included age, CRP and D-dimer levels on admission, history of hypertension and requirement of mechanical invasive ventilation. When adjusting for these confounders, therapeutic anticoagulation was associated with a lower risk of death (OR 0.079 95% CI 0.008-0.76).
When restricting the analysis for patients who required mechanical ventilation, anticoagulation was also associated with a lower risk of death (OR 0.031 95% CI 0.002-0.54) but not for intermediate doses (OR 0.10 95% CI 0.01-1.06).
(Figure 1)
Conclusions
Anticoagulation might not play a causal role in the risk of requiring mechanical ventilation, but the decision to increase doses might reflect patients who present with more severe disease. In our cohort, the majority of the patients were receiving intermediate prophylactic doses and the incidence of PE is lower than in worldwide reports. Therapeutic doses of anticoagulation were not associated with a lower risk of PE, but were associated with lower risk of death. However, therapeutic doses were also associated with a higher risk of major and clinically significant bleeding. Randomized-controlled clinical trials are needed to understand the role of higher doses of prophylactic anticoagulation in COVID-19.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal